The purpose of this webpage is to describe the most common diagnoses found during breast biopsy. When your doctor calls you with your breast biopsy results, this webpage may help you better understand your results.
BENIGN
Fortunately, most breast biopsies come back as "benign". This means that the biopsied area shows no signs of cancer or anything dangerous. When a biopsy comes back with one of these benign diagnoses, no treatment is usually necessary, and we usually recommend returning to routine yearly screening for women over age 40.
- Cysts are pockets of fluid that are found in the breast tissue of many women (about half of all women of child-bearing age have cysts). Cysts may be big or small and may even change size over time, but they are not dangerous and do not turn into cancer.
- Fibroadenomas are a normal part of the breast tissue in many women and are one of the most common results of biopsy. Fibroadenomas can grow slowly in some women, but they do not increase a women's risk of developing breast cancer. These typically do not cause symptoms and do not require any treatment, but larger fibroade-nomas can be removed if they cause discomfort.
- Fibrocystic changes is simply another form of normal breast tissue that may have a confusing appearance on imaging that prompts biopsy. It refers to a combination of tiny cysts (described above) and connective tissue.
- Fat necrosis can sound concerning but is just another term for how the breast heals from an injury to normal fatty breast tissue. Fat necrosis can be the result of trauma such as a car accident or surgery, or the injury may have been so minor that a woman may not remember the particular event. It can appear any time... even years after the injury. It represents a type of normal healing and never turns into breast cancer.
- Lymph nodes are a normal part of your immune system, and all women have lymph nodes in the armpit and often in the breast itself. Lymph nodes may change size due to infection or inflammation.
- Pseudoangiomatous stromal hyperplasia (PASH) is a benign type of tissue in the breast that does not turn into breast cancer. It may be look like a mass on a mammogram or may occasionally be felt as a lump. Despite the worrisome sounding name, PASH is benign and usually doesn't require any treatment at all.
INTERMEDIATE RISK
Biopsy results may show "intermediate risk" findings, which means no cancer is seen but the result is concerning enough that surgery may be necessary to remove the rest of the abnormal tissue (not the whole breast).
- Papillomas are small non-cancerous growths within a milk duct which may often cause nipple discharge or pain. Not all papillomas need to be removed. If the biopsy shows a papilloma with no atypical cells, then the papilloma usually does not have to be removed. We typically recommend follow-up imaging in 6-months for benign papillomas. But a surgeon may suggest surgical removal if the papilloma is causing bloody nipple discharge.
- Atypical papillomas have particular patterns to their cells that are more concerning than typical benign papillomas. We will frequently suggest removing atypical papillamas to make sure the pathologist has enough tissue to make an accurate diagnosis and to make sure it does not go on to develop into a form of breast cancer (most don't).
- Radial Scar (or Complex Sclerosing Lesion) are not scars and have nothing to do with trauma or injury. These are collections of milk ducts trapped in an area of twisted connective tissue. They can look just like breast cancer on mammograms or ultrasound, but they are not cancerous. However, in a small number of cases, unexpected breast cancers may be found near a radial scar. We recommend speaking with a breast surgeon about whether to surgically remove radial scars.
- Phyllodes tumors are rare tumors that are most often non-cancerous, but they tend to grow. In a small number of cases, phyllodes tumors may behave aggressively and spread to other sites in the body just like a cancer. We usually recommend surgical removal of phyllodes tumors.
HIGH RISK
Sometimes a biopsy shows "high risk" findings that do not appear to be cancer now but that are associated with a higher risk of getting breast cancer in the future. In a small number of cases, we may sample only a small part of pre-cancerous lesion or actual breast cancer, and the pathologist may only see enough to call it "high risk" but not enough to diagnose a cancer that is already there (this is uncommon). We recommend speaking with a breast surgeon about whether to surgically remove one of the high risk lesions listed here.
- Flat epithelial atypia (FEA) and atypical ductal hyperplasia (ADH) are often referred to as pre-cancerous lesions. They are considered one step away from the earliest forms of cancer and sometimes pathologists can have trouble distinguishing between ADH and DCIS (below). FEA and ADH should be removed as there is a small chance cancer cells may be found nearby and also because if left untreated they could turn into cancer in the future.
- Lobular carcinoma in situ (LCIS) and atypical lobular hyperplasia (ALH)are often grouped together and called lobular neoplasia. These high-risk lesions can signify an increased future risk of breast cancer and are typically treated with surgical excision.
CANCER / PRE-CANCER
Not all breast cancers are the same and different breast cancers will have different treatment options.
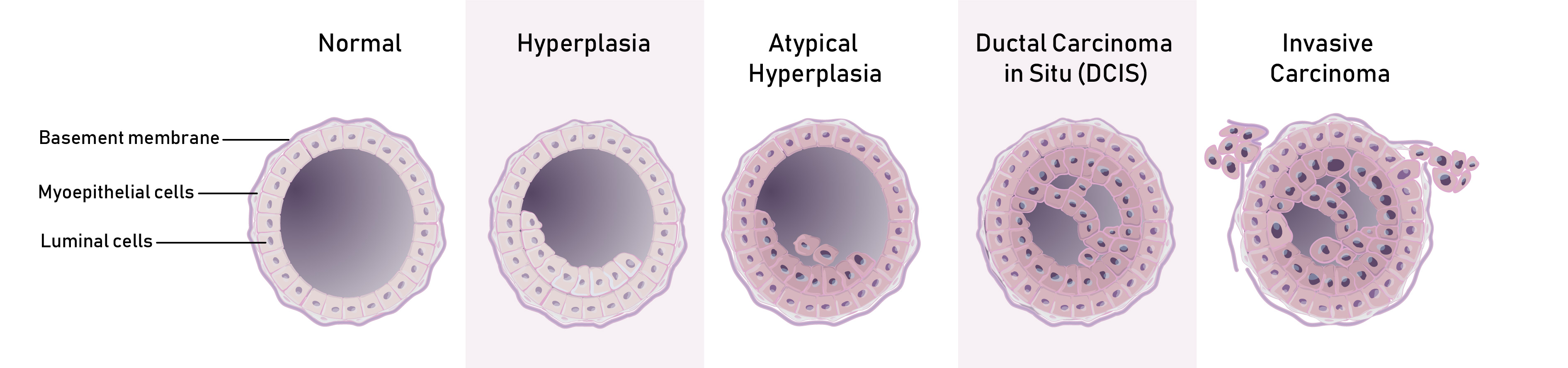
- Ductal carcinoma in situ (DCIS) means that abnormal cancer-like cells have started in the milk ducts but have not yet broken out of the milk duct into the surrounding breast tissue. This is sometimes called "pre-cancer". DCIS is frequently treated with surgical removal and often radiation therapy to the affected part of the breast, but research is being done at Duke and other centers to learn whether some cases of DCIS can be safely treated with a pill and close follow-up rather than with surgery.
- Invasive ductal carcinoma (IDC) is the most common form of breast cancer. Treatment for breast cancer will depend on how big it is and whether or not it has spread to the lymph nodes or other parts of the body. Treatment of breast cancer usually includes at least surgical re oval. Your doctors may also recommend chemotherapy and radiation therapy depending on the exact type of breast cancer.
- Invasive lobular carcinoma (ILC) is the second most common form of breast cancer. Treatment for this type of breast cancer is similar to the treatment for IDC (above). Invasive lobular carcinoma can be very difficult to see on mammogram, ultrasound or MRI, so it may be larger, but it is not more aggressive than the more common invasive ductal carcinoma.