
BEFORE THE PROCEDURE
It is necessary to have a recent pelvic examination and a normal pap smear by a gynecologist or primary care provider. For women with abnormal uterine bleeding or a thickened endometrial stripe on imagine, an endometrial biopsy should be done to rule out endometrial carcinoma or hyperplasia.
An MRI of the pelvis is obtained prior to visiting the Interventional Radiology (IR) physician. The MRI helps to determine whether or not a person is a candidate for UFE. During the visit with the IR physician, a thorough history and physical will be completed, the MRI imaging will be reviewed, and the procedural details will be discussed.
THE PROCEDURE
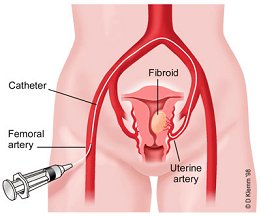
On the day of the procedure, an IV will be placed to administer sedation and any other medications. Once in the procedure room, an Interventional Radiology Technologist will scrub and drape the right groin area. Sedation will be given. The physician will then place a catheter into a femoral artery. This catheter will be directed into the arteries that supply blood to the uterus and ultimately the fibroids. When a safe catheter position is established, particles are injected to stop the flow of the blood to the fibroids. Once both uterine arteries are treated, the catheter is removed. This procedure usually takes less than 2 hours to perform. After the procedure is over, it is necessary to spend time in the recovery room before going to a private room for overnight observation.
RECOVERY
The most common complaints following UFE are menstrual-like cramps and nausea. To help keep the pain under control, a PCA (patient controlled anesthesia) pump is used to administer pain medication as needed. In addition to the pain medication, anti-inflammatory and anti-nausea medications are given.
Over 90% of women are able to go home the day after the procedure. After discharge, it is possible to experience continued cramping over several days. Pain medications can be prescribed to control these symptoms. The cramping typically lasts the same duration as a menstrual cycle with resolution within 7-10 days. An evaluation will be scheduled with the IR physician two to three weeks following the procedure.
BENEFITS
The earliest benefit is the brief time required for recovery following UFE. Patients typically are back to work and play within 7 to 10 days. For bleeding, our results and published reports confirm that greater than 90% of women will experience a decrease to a normal cycle. There is an 85% chance that the pain or bulk symptoms such as urinary frequency will improve. Greater than 80% of women will have a durable and effective resolution of their symptoms following UFE.
RISKS
About 2% of women completely stop having menstrual periods after uterine fibroid embolization. It remains unclear whether this is a result of decreased ovarian function from the procedure.
Adverse reactions are anticipated in less than 3% of women. Serious potential complications include injury to the uterus from decreased blood supply or infection. This is rare and hysterectomy (surgical removal of the uterus) to treat either of these complications occurs in less than 1% of women.
Long-term complications are uncommon, though several questions about potential side effects remain unanswered. It is uncertain what effect blocking the uterine arteries will have on the ability to become pregnant in the future, or to carry a pregnancy to full-term. The majority of women that have had this procedure are finished with childbearing, therefore only a few women have tried to become pregnant after this procedure.